No one is good at everything. Or bad at everything, for the most part. The majority of us are just about average. But neuropsychologists, specialists who test brain function for a living, expect a reasonable amount of scattering.
“In healthy humans, there is always some variability,” said neuropsychologist Victor Del Bene, Ph.D., assistant professor in the Department of Neurology in the UAB Heersink School of Medicine. The tests that Del Bene uses depend on a person’s age, their health and the cognitive issues they are experiencing. Memory concerns are a big one. Del Bene will use a battery of cognitive tests that may produce a dozen or more separate scores — in some cases, as many as 30. A typical battery covers “processing speed and reaction times, attention, language, visuospatial abilities, memory, and executive functioning,” Del Bene said. Most people will be better at some of these tests than others. “Even if you typically perform in the average range, not every score may hang together around the 50th percentile,” Del Bene said.
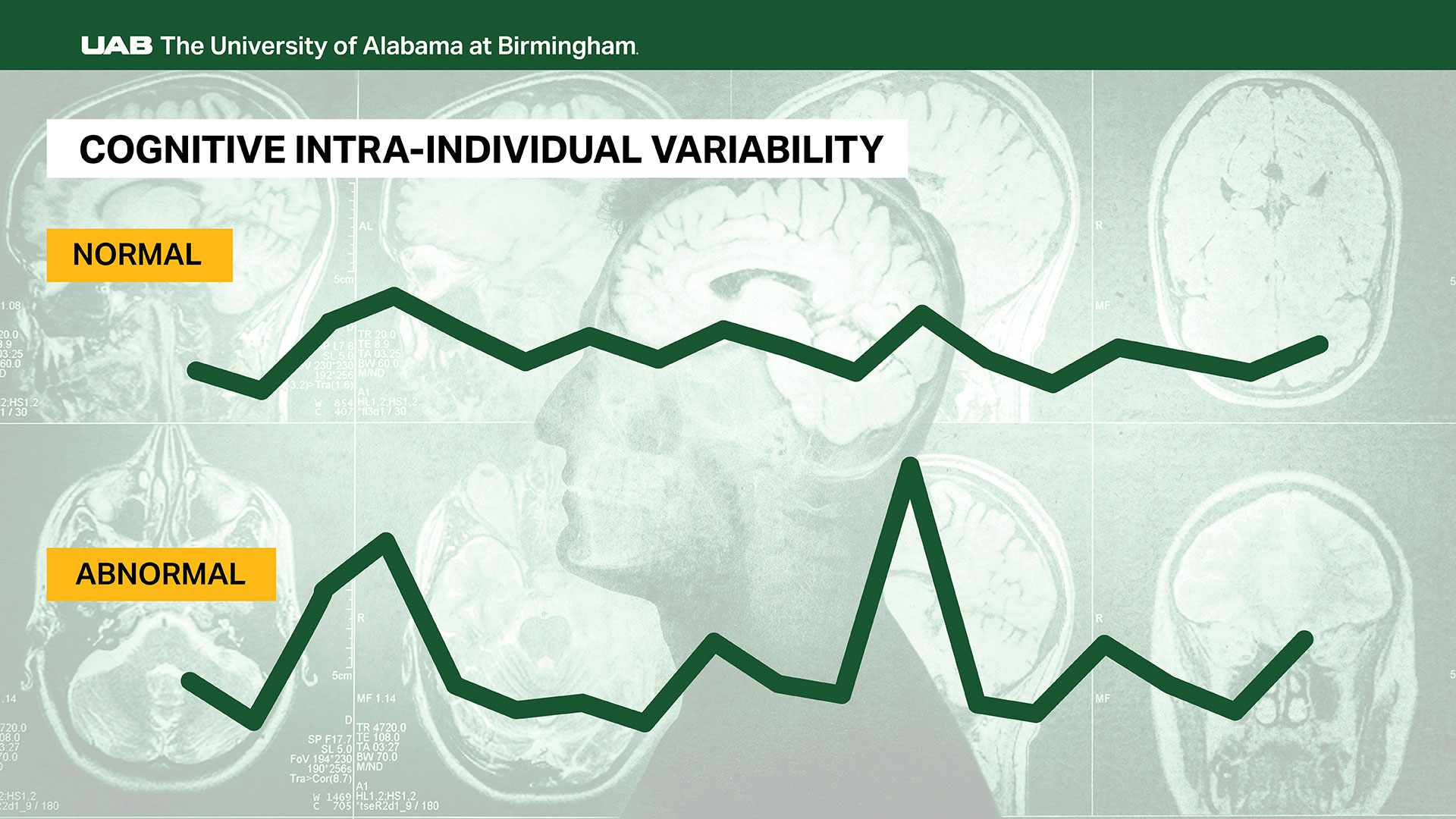
Still, research, including a paper co-written by Del Bene in 2023, demonstrates that people with healthy cognition generally have “coherent” scores on neurocognitive tests. That is, with enough tests, their scores fit the classic Bell curve, with nearly all of them clustered within one standard deviation of the center of the curve.
 UAB neuropsychologist Victor Del Bene, Ph.D., is one of a growing number of researchers studying cognitive variability.“You may have a few above and a few below that pattern; but what we know is that, when testing healthy people of average intellectual abilities, their scores tend to cluster together,” Del Bene said. “People with lower IQ scores have less variability, and those with high average IQs and above tend to have more variability in their cognitive profile.” It is unlikely, though, even with high IQs, that all scores will be in the superior range.
UAB neuropsychologist Victor Del Bene, Ph.D., is one of a growing number of researchers studying cognitive variability.“You may have a few above and a few below that pattern; but what we know is that, when testing healthy people of average intellectual abilities, their scores tend to cluster together,” Del Bene said. “People with lower IQ scores have less variability, and those with high average IQs and above tend to have more variability in their cognitive profile.” It is unlikely, though, even with high IQs, that all scores will be in the superior range.
“When you give 15 to 20 tests to healthy, high-functioning individuals, statistically it is likely you will get a few scores that are lower than expected, but do not fit a pattern of decline,” Del Bene said. “But when you introduce the presence of pathology, such as an ischemic brain injury or Alzheimer’s disease pathology, the variance in the cognitive profile starts to expand. Variability turns out to be a very sensitive marker to changes in brain function.”
A subtle sign that needs to be taken seriously
Del Bene is one of a growing number of researchers studying variability in individuals’ cognitive test scores, known as cognitive intra-individual variability, or IIV, meaning within-person variability.
In a new review paper in the journal The Clinical Neuropsychologist, Del Bene and co-authors, including David Vance, Ph.D., University Professor in the UAB School of Nursing, and Nicholas Borgogna, Ph.D., assistant professor in the UAB Department of Psychology, offer an overview of the history, methodology and future directions for study in the IIV field.
Intra-individual variability has been recognized for more than 100 years, Del Bene notes. But interest has taken off in the past decade or so.
Studies, including work by Del Bene and Vance, have shown that IIV is elevated in many different diseases. These include early-stage Alzheimer’s disease, HIV infection, Parkinson’s disease, frontotemporal dementia, traumatic brain injury, Lewy body disease, neuroinvasive disease, schizophrenia, depression and breast cancer.
"Variability turns out to be a very sensitive marker to changes in brain function.”
“Elevated IIV has been found to predict progression from normal cognitive status to mild cognitive impairment and dementia, as well as risk of functional decline [i.e., difficulties with financial management] and increased risk of morbidity and mortality,” Del Bene and his co-authors wrote.
A recent meta-analysis led by Stephen Aita, Ph.D., and co-written by Del Bene, showed consistent patterns in Alzheimer’s research of increased IIV in people with mild cognitive impairment and even more IIV in people with dementia due to Alzheimer’s disease.
“Cognitive intra-individual variability could be particularly helpful in diagnosing early-stage neurodegenerative disease, when patients come in with subjective concerns and some lower scores on testing but nothing in the impaired range,” Del Bene said. “Variability can be a subtle sign that needs to be taken seriously. With emerging biomarkers for Alzheimer’s disease, subjective cognitive concerns paired with cognitive variability may be sufficient to refer a patient to clinics specialized in memory disorders.”
Calculating cognitive intra-individual variability
When interpreting cognitive scores, neuropsychologists compare a patient’s test scores to the scores from the normative sample. That is, scores from people of the same age and other shared demographic adjustments, who should have roughly equal performance. In the absence of baseline assessments, or earlier test results from the same patient, this is the gold standard approach for an initial assessment.
If there is a clear pattern of memory test scores’ being much lower than expected, that is a cause for concern and further evaluation, including referral to a neurologist and a brain MRI or PET scans. But what if no scores drop below that threshold?
This happens more often than you might think. When Del Bene was a postdoctoral fellow, participating in morning patient reports in the clinic, he noticed how often his mentors would debate whether the variability they were seeing in a patient’s neuropsychological profile was normal or was indicative of an emerging pathology, medical illness or other psychological factors. “Trying to disentangle this question became an interest of mine,” Del Bene said. “How do we figure out what is normal and what is abnormal variability?”
Del Bene trained under mentors at Johns Hopkins University, who opened his eyes to the importance of cognitive IIV.
“Cognitive intra-individual variability could be particularly helpful in diagnosing early-stage neurodegenerative disease, when patients come in with subjective concerns and some lower scores on testing but nothing in the impaired range.”
At its core, IIV is focused on fluctuations in performance. That could be inconsistent results on a single test or how scores are dispersed across a battery of tests. One common formula for IIV starts by calculating a person’s average performance across a test battery, known as the overall test battery mean, then determines the standard deviation around that mean. To account for the overall test battery average, you can then divide the standard deviation by the overall test battery mean, yielding a score called the coefficient of variation. Other approaches, as outlined in the 2023 paper co-written by Del Bene, use statistical approaches of skewness and kurtosis to capture the variability seen in the cognitive profile.
Abnormal fluctuations in performance are a clue that something is going wrong. Imagine three memory tests are administered. One is within normal limits, one is in the impaired range, and one is on the cusp of normal and impaired, or borderline impaired. This could be a clue that the part of the brain associated with memory is not functioning as well as the rest.
Why can’t we be consistent?
For more than a century, psychologists have been puzzled by the phenomenon of variability. “Early experimental psychology and psychophysics research using reaction times looked at why people were not consistent in their responses,” Del Bene said. Given the technology of the time, the most visible way to measure this was on tests of reaction time, but technological limitations made it challenging to study this accurately, since measurement of reaction times needs to be at the millisecond level.
In the 1990s, “some people returned to this idea, and we started seeing that this phenomenon is quite sensitive,” Del Bene said. “It is telling us something unique, and it turns out it can tell you a lot about brain function.” From 1977 to 2000, there were only 24 studies that referenced IIV; but between 2001 and 2025, that number has jumped to 667 studies, showing the growth in research interest, Del Bene notes.
In their new paper, Del Bene, Vance and their co-authors summarize where the field is now and what is next.
A 2023 paper by Vance, with Del Bene as co-author, examined multiple studies of IIV in breast cancer survivors. “The four studies provide support for cognitive IIV as a useful measure to detect the subtle objective cognitive change often reported by breast cancer survivors but frequently not detected by standard normed-based cognitive testing,” the authors wrote.
Another clinical application of cognitive intra-individual variability measures could be to measure the impacts of rehabilitation. “Patients do recover cognitively from stroke and traumatic brain injury,” Del Bene said. “IIV could potentially also tell us about the healing process.” In a 2024 paper, Vance and co-authors report that IIV was reduced in some participants following cognitive training, suggesting there may be validity to the claim that IIV can also be used to track cognitive improvement after an injury.
What neuropsychologists can do with IIV
“If a patient comes in with subjective concerns and I’m seeing that they are not necessarily impaired but there is variability dispersed across the profile and they are engaged on testing, that raises a yellow flag.”
Although there are no standardized guidelines for using IIV in the clinic, the field is heading in this direction. Del Bene’s colleague Andrew Kiselica, Ph.D., a neuropsychologist at the University of Georgia, recently developed a normative dataset for IIV in patients with Alzheimer’s disease based on data from National Alzheimer’s Coordinating Center, which curates a publicly available dataset from Alzheimer’s Disease Research centers around the country. “The purpose of Dr. Kiselica’s study was to figure out what is normal versus abnormal IIV in a sample of healthy participants,” Del Bene said. With this dataset as a reference, Del Bene has a better idea for when a patient’s IIV “is pathologically elevated, which is really helpful,” he said.
“If a patient comes in with subjective concerns and I’m seeing that they are not necessarily impaired but there is variability dispersed across the profile and they are engaged on testing, that raises a yellow flag,” Del Bene said. “During feedback with the patient, I’ll make recommendations to address lifestyle factors and behaviors that may be contributing to the cognitive variability, and I’ll ask them to return for a repeat assessment in six months or 12 months so that we can keep an eye on that variability. At the return visit, if I see increased scatter in the scores, or the trajectories of cognitive domains are now starting to show decline and they addressed behaviors such as sleep, depression or blood pressure, then IIV was helpful in the early detection of these cognitive symptoms. Depending on the underlying cause of IIV and decline, we can then refer the patient for biomarker and advanced imaging workup, to the sleep clinic, or provide further behavioral recommendations, such as exercise or psychotherapy.”
At this point, “there’s a lot of work that shows that IIV is very sensitive to pathology versus non-pathology,” Del Bene said. “Now we are starting to go further, with biomarker research and imaging research.” In February 2026, Del Bene and his collaborators submitted a new paper (available now as a pre-print) that correlates IIV scores with cerebrospinal fluid biomarkers and amyloid PET in people with mild cognitive impairment and dementia. No association was seen with the presence of Alzheimer’s disease biomarkers and IIV in the cognitively unimpaired group.
“Calculating IIV will not and should not replace traditional methods of scoring and interpreting cognitive tests,” Del Bene said. “But IIV may be another tool in the toolbox, especially for difficult borderline cases where there may be subtle changes early on.”