Case History:
A 55 year old female patient underwent MRI guided biopsy for a non-mass enhancement. She has previously biopsy-proven ipsilateral breast carcinoma.
What is the most likely immunohistochemical profile of this lesion?
A. ER positive, PR positive, HER2 positive.
B. p63 positive, smooth muscle myosin heavy chain positive.
C. S100 positive, CK CAM5.2 positive, ER/PR negative, myoepithelial cell markers negative.
D. GCDFP-15 positive, androgen receptor (AR) positive.
Correct answer: C. Microglandular adenosis.
Discussion
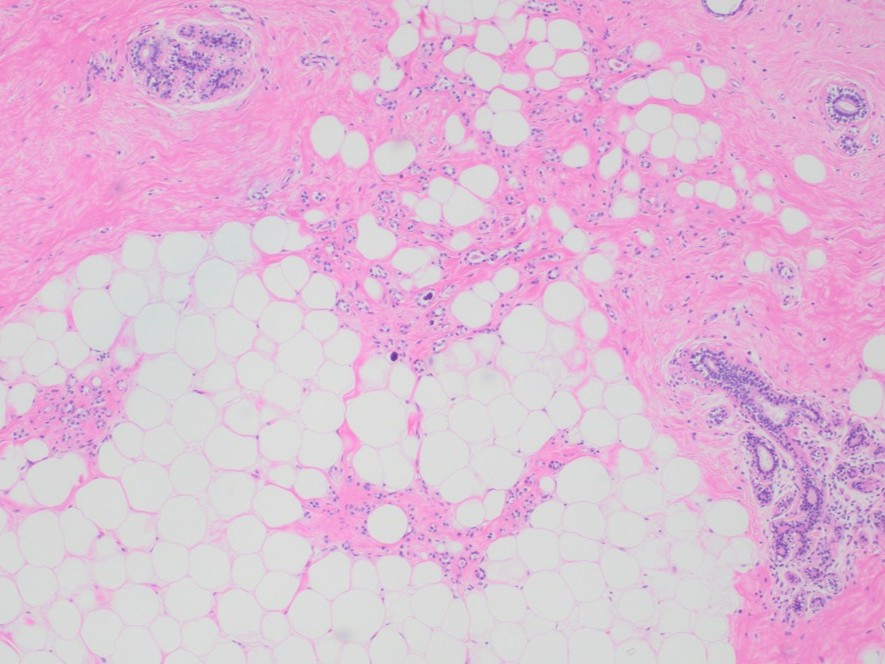
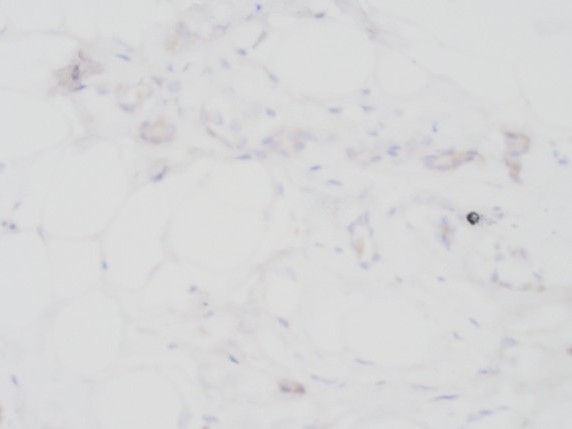
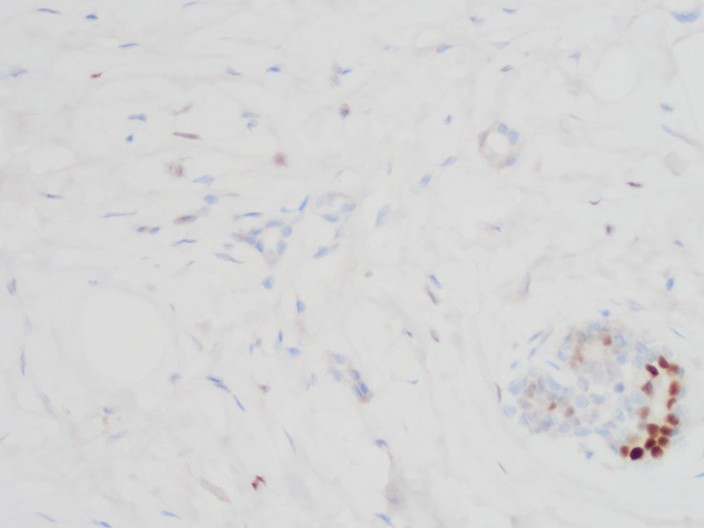
Microglandular adenosis (MGA) is characterized by small uniform glandular proliferation with open lumen and frequently containing amorphous eosinophilic material. Lesion is usually poorly circumscribed, with the proliferating glands permeated into the surrounding normal breast tissue and adipose tissue. Glands are lined by one layer of cuboidal epithelial cells surrounded by basal lamina without evidence of myoepithelial cell layers. Studies have shown MGA is strongly positive for low molecular weight keratin and S100; and consistently negative for estrogen receptor (ER), progesterone receptor (PR), and HER2. Collagen IV and laminin-positive well-formed basal lamina are seen. Most significant differential diagnoses include sclerosing adenosis (with a lobular centric pattern and positive myoepithelial cell layers), and tubular carcinoma (ER/PR positive, negative for basal lamina, with stromal desmoplastic changes, and usually S100 negative). Over the years, numerous studies have reported that MGA appeared to be associated with carcinomas, either with atypia, malignant transformation of triple-negative neoplasm or as an innocent bystander, among which, acinic cell carcinoma was emphasized. Treatment of biopsy identified MGA is excisional biopsy.
Case contributed by: Hua Guo, M.D., Associate Professor, Women's Health