Three faculty members in the Department of Psychology are getting ahead in the race to end chronic pain.
By Gigi DoubanPhotos by Nik Layman
A broken bone shows up on an X-ray. An MRI can reveal a tumor. But what does pain look like? Come to think of it, what is pain, really? The person experiencing it has no doubt it’s there, and can usually describe it—sharp, throbbing, dull, comes-and-goes. But unless it’s taken as part of a cluster of symptoms to some other illness, some in the medical community are quick to trivialize chronic pain as not a real thing, as something that’s in the patient’s head.
The common perception that chronic pain is imagined, or not serious, persists despite the fact that about 100 million American adults live with chronic pain, according to the Institute of Medicine. It affects more people than diabetes, cancer, and heart disease combined. “People are getting older, living longer,” says Dr. Burel Goodin, Assistant Professor of psychology and anesthesiology. That means more people are dealing with persistent pain issues.
Pain is also among the least understood public health issues. A small group of UAB researchers is trying to change that. Through the work of Dr. Robert Sorge, Dr. Jarred Younger, and Goodin, UAB is establishing itself as a pain research powerhouse. Together, these researchers are unlocking some of the mysteries that surround chronic pain, redefining the illness in its own right, and developing cutting edge ways to treat it.
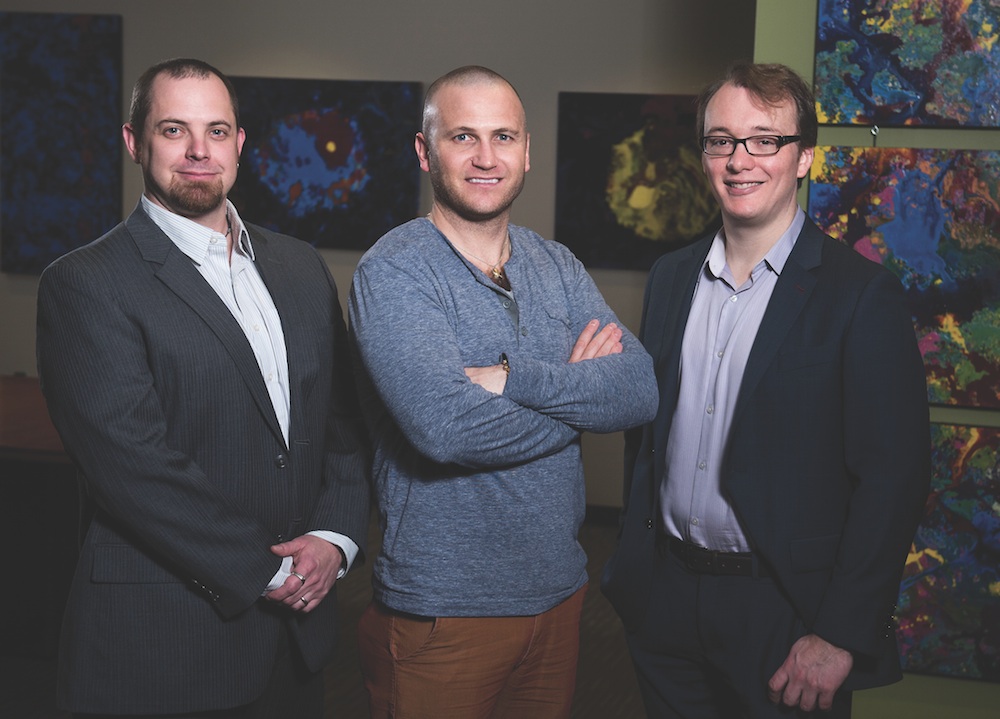 From left: Dr. Robert Sorge, Dr. Burel Goodin, and Dr. Jarred Younger.
From left: Dr. Robert Sorge, Dr. Burel Goodin, and Dr. Jarred Younger.It’s time, says Goodin, Assistant Professor of psychology and anesthesiology. “Prior to two and half years ago, none of us was here. There wasn’t really this large pain presence,” he says. “What we’re trying to get is this nice critical mass of pain researchers. And once we do, who knows? We may end up getting some cool pain-related center. The interest is really there..
Chronic pain is probably the most expensive problem in the U.S., says Younger, Associate Professor and director of UAB’s Neuroinflammation, Pain, and Fatigue Lab. Some estimates put it as high as $635 billion a year. That’s more than heart disease, diabetes, or cancer.
The work being done at UAB is triggering a shift in the way people think about chronic pain. People usually think of acute pain. “I stubbed my toe. That hurts. That pain is a symptom of stubbing my toe,” Goodin says. But more and more, those in the health sphere are beginning to consider chronic pain its own disease entity.
Connecting Food/Pain
What you eat affects the way you sense pain, and how quickly you recover from injury. That’s the crux of Robert Sorge’s research, which involves feeding mice what Sorge’s lab calls a Western diet: meals high in refined carbohydrates, saturated fats, and trans fats. “We’re looking at what a poor diet does to our animals over the long term in terms of their sensitivity to painful stimuli and their recovery from a chronic pain condition,” he says.
Dr. Robert Sorge
Obese people, he says, can withstand the pain of a hot metal disc placed on the arm a little longer than most. Is it a matter of more fat providing more padding? “It shouldn’t be,” Sorge says. Our pain receptors are right on the skin. “What we’re thinking is happening is that obesity and a poor diet lead to this chronic inflammatory state,” he says.
What’s wrong with being less responsive to acute pain? Animals in this chronically inflamed state show higher levels of pro-inflammatory cytokines, chemical messengers released by immune cells. And there’s a disruption in circuitry that happens here.
We have two types of pain neurons: one is the rapid response, which is that immediate shock when you first put your hand on something hot. The second is non-myelenated, which responds to dull, throbbing, aching pain. Think about a toothache or the pain after twisting your ankle.
“What we’re thinking is happening is that obesity and a poor diet lead to this chronic inflammatory state.”
— Robert SorgeWhen Sorge induces an arthritic state in mice, in most, it’ll last about a week before they’re back to normal. But the animals fed a poor diet show more sensitivity to this type of pain, and recovery takes almost twice as long, up to 14 days. “And in obese patients, we see something very similar,” Sorge says. So a person of normal weight might feel pain from a strained back for three to five days. “Someone that’s obese may have the same injury, feel more pain, and it may take them a week or two to recover from it.”
For a long time, the immune system and inflammation were thought to be completely separate. “Now we know they’re one and the same,” Sorge says. Immune cells release these proinflammatory cytokines and cause inflammation. “We’re looking to see how this poor diet changes the functioning of your immune system. That’s where we are now.”
Ultimately, Sorge hopes to see if anti-infammatory foods, like those containing grapes, ginger, broccoli, leafy greens, and curcumin from turmeric root can reverse that effect. High levelsof carbohydrates trigger inflammation, and fat deposits release a hormone called leptin, which also leads to inflammation. Sorge is beginning a human clinical trials to look at the effect of dietary changes on pain levels and inflammation.
Study participants will fall into one of three groups: a low-carbohydrate diet, a low-fat diet, and a control group. Sorge is recruiting older adults with knee osteoarthritis who will keep a food diary and rate their pain weekly. “We’re expecting weight loss in both groups, but we’re hoping to see that it’s the diet and not necessarily the weight loss that has the bigger effect,” he says.
It’s thought that a lot of the chronic pain issues faced by obese individuals stem from having extra weight to stress the joints and muscles. Sorge says that’s not the whole picture. “They also tend to have a lot of inflammation in the neck, in the shoulders, in the fingers, which are not significant weight-bearing joints,” Sorge says. “That suggests it’s not the weight, it’s something about the obesity itself.”
Ending Inflammation
When a person gets the flu, it activates the immune system. “When immune cells in our brain detect a virus, they release a bunch of chemicals that make us feel sick,” says Jarred Younger. But think about the symptoms. “You’re going to be sensitive to pain, you’re going to want to lay in bed all day, you’re not motivated to do anything, your mood’s depressed, you don’t feel like interacting with people,” he says. “It affects every level of your being.”
Dr. Jarred Younger
Microglia are cells that are constantly patrolling for problems in the brain, including viruses and bacteria. When they detect a problem, they activate. But in people with chronic pain, they go into attack mode even without a problem. “The thing that can trick it, that’s the part we’re still trying to figure out.”
There are dozens, maybe hundreds of things that can sensitize those cells, Younger says—aging makes them more sensitive, which could be why older adults are more easily fatigued and experience cognitive declines; lots of infections, long-term exposure to diesel particles in the air, chronic stress, obesity—all of these things make these cells go into attack mode.
Younger is developing drugs that get into the brain and reduce inflammation. “So we’re testing drugs that go to the microglia and it suppresses them.” The theoretical risk is that if you turn off these cells too much, they won’t be there when you need them. “So we have to be sure that we’re not overly suppressing the immune system,” he says. In the human trials he’s conducted so far, he says, there’s no evidence to suggest that’s happening.
Current pain treatments—opioid painkillers—are addictive and potentially deadly. They’ve been reformulated so they last longer, but it’s still the same basic idea, Younger says—they’re not treating the cause of the pain. It’s a challenge to treat pain unconventionally, he says. “We certainly aren’t doing mainstream stuff,” he says, “but that’s how you make major advances.”
“We certainly aren’t doing mainstream stuff, but that’s how you make major advances.”
— Jarred YoungerAnd Younger, backed by the Department of Defense, is looking at what’s behind the strange symptoms reported by veterans of the 1991 Persian Gulf War. Those soldiers, he says, were exposed to experimental vaccines and oil fumes. “So we’ve got all these people with chronic disease, and now the government’s really invested in trying to figure out what happened and how do we cure it.”
Younger’s lab is also experimenting with Chinese botanicals, ranging from turmeric-derived curcumin to mushrooms—to test their effect on inflammation.
No Two Pains Are the Same
Things that hurt one person might not hurt another. “And things that hurt both of us don’t necessarily hurt somebody else,” says Burel Goodin. “And because no two pains are created equally, I’ve always been interested in, ‘Well, why is that?’” Dr. Burel Goodin
Dr. Burel GoodinGoodin has exposed people to a sad stimulus—have them watch a sad video, for example—or made them feel socially excluded and rejected in the lab. “So maybe that rejection hurt emotionally,” Goodin says. “What I’m often interested in is does that emotional hurt map onto their physical hurt?” A lot of times, Goodin says, it does.
“We make this arbitrary distinction between physical hurt and emotional hurt, but the brain itself really only knows ‘hurt,’” he says. The same area of the brain that lights up when a person is rejected and emotionally hurt is the same part that responds when a person is poked with a sharp object.
Individual differences in the experience of pain often have something to do with learned experiences. These can be related to gender (think of the difference in how adults react when a little girl skins her knee versus a little boy), to experiences shared by members of certain racial or ethnic groups.
Goodin published a study in 2012 looking at African-Americans’ pain sensitivity. He found that among people who report having been discriminated against, whether in a medical setting, looking for housing, or by the police, they were more sensitive to pain. “Particularly among African-Americans, the more they reported being exposed to racial discrimination, the less they were able to tolerate a painful stimulus,” Goodin says.
“We make this arbitrary distinction between physical hurt and emotional hurt, but the brain itself really only knows hurt.”
— Burel GoodinFor people who are stigmatized or routinely discriminated against, Goodin’s goal is to help them cope. “Trying to increase their resilience, trying to up their threshold for tolerating these things,” he says. That might involve connecting them with resources such as social support networks or teaching them relaxation techniques.
In the end, he says, the work that he, Younger, and Sorge are doing together is helping form a clearer picture of what it means to experience chronic pain. “So what is ultimately impacting their pain? Is it psychological or is it physical? My answer is ‘yes.’”


